In the very crowded area of airway management
for anesthesia and critical care medicine several
authors reported interesting comparison among
the different techniques to perform a rapid and
safety intubation for routinely approach or unexpected difficulty.
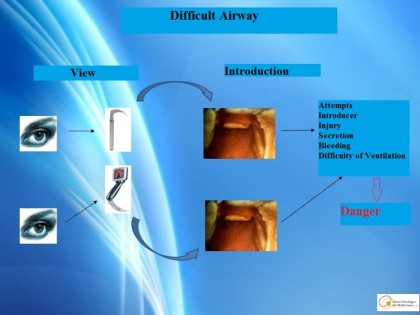
Recently Takashi Asai focuses the role of techniques vision based
in the solution of problems with tracheal intubation.
The essential message coming from Takashi Asai
signify that the entire intubation procedure
requires visualization of the vocal cords and
that the endotracheal tube should be introduced
under visual control.

Under general anesthesia, the entire tracheal intubation
procedure should be carried out under visual control to limit the risks.
Recently, many devices have been developed that
allow laryngeal visualization.

But these are limited to the first stage of the procedure,
i.e., visualization of the glottis.
The second phase, insertion of the
endotracheal tube, is sometimes performed blind,
which carries a risk of trauma and bleeding.
The only instrument that provides full visualization
throughout intubation is the flexible bronchoscope.
In our Oncologic Institute, we often encounter patients
who have cancers located in the head and neck regions,
necessitating the use of a flexible bronchoscope.
Under conditions of anesthesia with muscle relaxation,
the use of a flexible bronchoscope can be difficult.
Thus, we have developed an intubation technique
that uses a flexible bronchoscope in combination
with the MacIntosh laryngoscope under anesthesia
with muscle relaxation for unexpected difficult intubations .
The MacIntosh laryngoscope acts as a lever, allowing
for normal maneuvering of the bronchoscope under anesthesia.
This technique has allowed successful intubation
even in cases with laryngeal visualization of Cormack grade 4
The procedure was performed successfully by an
experienced anesthesiologists in 200 hundred
surgical patients.
The ethics committee approved the standardization
and the method for training the young anesthesiologists
in the use of the combined intubation technique.
We started a cooperative project with the Medical School
of Anesthesiology in Catania for training
the fellows under the tutor guidance.
The results obtained from a comprehensive 314
surgical procedures involving the neck, abdomen, breast,
and spinal cord are encouraging .
Using an algorithm that uses the combined technique
in cases of Cormack-Lehane grade 3 and up ,
no attempts were made at blind intubation.
Instead, the combined technique was used
successfully in 51 cases out of 51.
Our technique should be performed by other teams
to confirm its efficacy. Owing to its simplicity
and low cost, this combined method could simplify
intubation under general anesthesia with muscle relaxation,
and it is our experience that it can be learned
quickly by novice operators. In our practice,
it has taken an average of ten procedures for
a novice to reach proficiency.
References
1) Asai, T: Videolaryngoscopes: do they truly have roles in difficult airways? Anesthesiology 2012 Mar; 116(3): 515–7